Χονδροπάθεια Επιγονατίδος
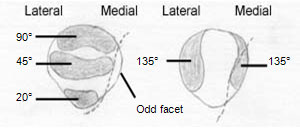
Η Ανατομική του Γόνατος
Η Χονδροπάθεια του Γόνατος είναι μια συχνή επώδυνη πάθηση των γονάτων. Στην αμερικανική και αγγλική βιβλιογραφία, η πάθηση αυτή αναφέρεται με τον όρο Pattelofemoral Stress Syndrome το οποίο εμπεριέχει την Χονδροπάθεια Επιγονατίδος την Χονδροπάθεια των Μηριαίων κονδύλων αλλά και τις Τενοντίτιδες του τετρακέφαλου και του Επιγονατιδικού συνδέσμου.
Παθολογική Ανατομική
H Χονδροπάθεια του Γόνατος προσβάλει κυρίως τον χόνδρο της επιγονατίδας και κατά δεύτερο λόγο το χόνδρο της Μηριαίας τροχιλίας. Ο χόνδρος των Κνημιαίων κονδύλων δεν είναι εύκολο να φθαρεί γιατί προστατεύεται από τους δύο Μηνίσκους, οι οποίοι όταν φθαρούν ή αφαιρεθούν οδηγούν σε φθορά του χόνδρου των Κνημιαίων κονδύλων.
Επιδημιολογία
Η Χονδροπαθεια της επιγονατιδας, είναι συχνή επώδυνη πάθηση του γόνατος η οποία εκδηλώνεται συνήθως σε νέα άτομα από 15-40 ετών. Προσβάλλει περισσότερο τις γυναίκες παρά τούς άνδρες, σε αναλογία 3:1. H Χονδροπάθεια είναι πιο συχνή από τούς τραυματισμούς των Μηνίσκων, αλλά συνήθως παραμένει ασυμπτωματική στην εφηβική ηλικία, διότι αυτοϊάται με σχηματισμό ινώδους χόνδρου. Η πάθηση είναι αρκετά συχνή ακόμα και σε άτομα εφηβικής ηλικίας. Υπολογίζεται ότι το 80-85% του πληθυσμού στην ηλικία 20-30 έχει εκφυλιστικές αλλοιώσεις και βλάβες του χόνδρου της επιγονατιδομηριαίας αρθρώσεως
Αιτιολογία
Η Χονδροπαθεια της επιγονατιδας, οφείλεται σε είτε σε τραυματισμό, είτε σε χρόνια υπερφόρτιση του χόνδρου της Επιγονατίδας, είτε σε εσωτερικούς παράγοντες γενετικής προδιάθεσης («ευπάθειας») του αρθρικού χόνδρου, είτε σε συνδυασμό αυτών. Γενικά, η πάθηση είναι πολυπαραγοντική, οφείλεται δηλαδή σε συνδυασμό πολλαπλών αιτίων, τά οποία χωρίζονται σε ενδογενή και εξωγενή .
Στάδια
H Χονδροπάθεια του Γόνατος έχει τρία παθολογοανατομικά στάδια:
Στάδιο Ι: Οίδημα του Χόνδρου με κιτρινόφαιες μαλακές και προεξέχουσες εστίες χωρίς καμία ελαστικότητα και κάμψη.
Στάδιο ΙΙ: Ρωγμές και «ξεφτίσματα» του χόνδρου. Ελεύθερα χόνδρινα σωμάτια στο αρθρικό υγρό και αλλοιώσεις χρόνιας Υμενίτιδας.
Στάδιο ΙΙΙ: Ελκη κατά τόπους στον χόνδρο. Το υποχόνδριο οστό είναι ακάλυπτο στον πυθμένα τους και υπόσκληρο.
Συμπτώματα και κλινική εικόνα
Συνήθως, μετά από κάποιο τραυματισμό της Επιγονατίδας, ή από χρόνια υπερκαταπόνηση σε εργασία σε γονατιστή θέση, ή σε γυμναστήριο, ή χορό, ή σε πεντάλ τροχοφόρων, πρέπει να περάσουν 3-6 μήνες ώσπου να εκδηλωθούν τά φαινόμενα της Χονδροπάθειας στον ασθενή. Ο ασθενής αναφέρει ότι «έχει ένα πόνο μπροστά στα γόνατα», ότι «αισθάνεται ένα κάψιμο», ότι «ακούει ήχους κράκ στο γόνατο», ότι «του φεύγει το γόνατο στο κατέβασμα σκαλοπατιών» (σημείο Giving way), ότι «θέλω να τεντώνω τα γόνατά μου», ότι «δυσκολεύομαι να κάνω βαθύ κάθισμα», ότι «δυσκολεύομαι όταν σηκώνομαι μετά από πολλή ώρα καθίσματος» («σημείο κινηματογράφου»), κλπ. Η Χονδροπάθεια επιγονατίδων διαγιγνώσκεται με το ιστορικό και με την κλινική εξέταση με τα χέρια. Το πλέον αξιόπιστο τέστ είναι η "δοκιμασία ολίσθησης και πλάγιας μετατόπισης της επιγονατίδας" πάνω στη μηριαία τροχιλία, με το γόνατο σε έκταση και χαλαρό, οπότε αναπαράγεται κριγμός και πόνος. Αλλα κλινικά ευρήματα είναι οι προκλητοί πόνοι στα χείλη της επιγονατίδος, η ύπαρξη υδράρθρου και υμενίτιδας, το "Τest Zohlen" (πόνος σε σύσπαση τετρακεφάλου) και το "σημείο αναπήδησης", που είναι το απότομο τίναγμα της επιγονατίδας σε κάμψη 30-40 μοιρών
Απεικονιστικός έλεγχος
Η πάθηση δεν φαίνεται στις απλές ακτινογραφίες. Το μόνο που προσφέρουν είναι η απεικόνιση κατασκευαστικών ανωμαλιών όπως η υψηλή θέση της επιγονατίδος, η αβαθής Μηριαία Τροχιλία, η Διφυής Επιγονατίδα, η έξω θέση της Επιγονατίδας, η ύπαρξη κύστεων, τυχόν ύπαρξη οστεοφύτων, κλπ. Ενίοτε βοηθάει διαγνωστικά η CTκαι η MRI, αλλά δεν μπορεί πάντα να απεικονίσει τις αλλοιώσεις του χόνδρου. Η Αρθροσκοπηση είναι η άριστη μέθοδος για τεκμηρίωση της διάγνωσης, αλλά απαιτεί γενική νάρκωση και νοσηλεία μιάς ημέρας. Πάντως, με το καλό ιστορικό, την καλή κλινική εξέταση και τις ακτινογραφίες, η διάγνωση τίθεται με βεβαιότητα 65% στο 1ο στάδιο και 80% στο στάδιο ΙΙ, χωρίς άλλες εξετάσεις
Θεραπεία
Ελαφρές περιπτώσεις χονδροπάθειας επιγονατίδας συνήθως αυτοθεραπεύονται μέσα σε 30-45 μέρες. Τα περιστατικά ασθενών, αντιμετωπίζονται με αδυνάτισμα σε παχύσαρκους, ελαστική περιγονατίδα με οπή, ανάπαυση, αποφυγή καταπόνησης σε σκαλοπάτια ή έντονη άθληση, αντιφλεγμονώδη φάρμακα (για τον πόνο και το οίδημα), και ανακουφιστικές φυσικοθεραπείες. Το ποδήλατο με μεγάλη κάμψη γόνατος βλάπτει. Οι ασκήσεις τετρακέφαλου δεν πρέπει να ξεπερνούν τις 30 μοίρες, στην οξεία κρίση της παθήσεως Μεσαίας βαρύτητας περιστατικά χρειάζονται 5 ενδαρθρικές ενέσεις Sodium Hyaluronate,. H χρήση του Υαλουρονικού Νατριου από το έτος 1997 στήν Χονδροπάθεια Επιγονατίδος απεδείχθη λίαν επιτυχής. Φαίνεται να αναστέλλει τις βλάβες αλλά και να διευκολύνει την επούλωση στις ήδη προϋπάρχουσες, με αποτέλεσμα τα τελευταία χρόνια να έχουν σχεδόν εξαφανισθεί οι εγχειρήσεις γιά θεραπεία Χονδροπάθειας.
Σοβαρές περιπτώσεις Χονδροπάθειας της Επιγονατίδας μάλλον δεν θεραπεύονται ποτέ 100%, αλλά αρκετά θεραπευτικά μέτρα είναι αποτελεσματικά για την ανακούφιση των ασθενών. Η θεραπεία χρειάζεται, όχι μόνο γιατί πονάει ο ασθενής, αλλά γιατί σταδιακά οδηγεί τα προδιατιθέμενα άτομα σε Οστεοαρθριτιδα του γόνατος. Τα άτομα αυτά χρειάζονται συνήθως Επεμβαση αρθροσκόπησης, με τρυπανισμούς για αναγέννηση χόνδρου, διατομή έξω καθεκτικού συνδέσμου, κλπ. Τα τελευταία χρόνια εφαρμόζεται πειραματικά και η αυτόλογη μεταμόσχευση καλλιεργημένων χονδροκυττάρων του ασθενούς μέσω διαδικασίας αρθροσκόπησης, όμως η μέθοδος απαιτεί τρείς εγχειρήσεις αρθροσκόπησης υπό γενική αναισθησία. Εκτος αυτου μπορούν να γίνουν εξειδικευμένες διορθωτικές χειρουργικές επεμβάσεις. Μερικές από αυτές είναι η "εγχείρηση Maquet" (ανύψωση Κνημιαίου Κυρτώματος), η εγχείρηση διατομής έξω καθεκτικού συνδέσμου, η μηχανική λείανση του χόνδρου, οι τρυπανισμοί, κάθετοι και πλάγιοι, η εκτομή της Υμενικής πτυχής, η οστεοτομία της επιγονατίδος,
ΦΥΣΙΚΟΘΕΡΑΠΕΥΤΙΚΗ ΠΡΟΣΕΓΓΙΣΗ
Η θεραπεία περιλαμβάνει τρία στάδια:
• Αντιμετώπιση της οξείας φάσης
• Αποκατάσταση
• Πρόληψη
• Αποκατάσταση
• Πρόληψη
Στην αντιμετώπιση της οξείας φάσης, όπως συμβαίνει σε όλα τα σύνδρομα υπέρχρησης, πρέπει ο ασθενής να διακόπτει όλες εκείνες τις δραστηριότητες που του προκαλούν πόνο. Σε αυτήν την φάση εφαρμόζουμε τεχνικές για την ελάττωση της φλεγμονής, όπως είναι η θεραπεία με Laser, ιοντοφόρεση με διάλυμα solu-medrol και xylocaine 2%, παλμικό μαγνητικό πεδίο (διεισδύει στο σώμα ομοιόμορφα, ανεπηρέαστο και επιδρά στην ενδοκυτταρική κίνηση των ιόντων, αυξάνει δηλαδή την διαπερατότητα της κυτταρικής μεμβράνης, με αποτέλεσμα την ελάττωση του οιδήματος και του πόνου, γρήγορη απομάκρυνση των προϊόντων του μεταβολισμού, αύξηση της παροχής του οξυγόνου στην περιοχή), ειδική επίδεση του γόνατος, ώστε η επιγονατίδα να συγκρατείται σε σωστή τροχιά κίνησης, ενώ σύμφωνα με το αποτέλεσμα του πελματογραφήματος ο ασθενής άμεσα πρέπει να φορά στα παπούτσια του ειδικά κατασκευασμένα πέλματα, ώστε να εξισορροπούνται οι δυνάμεις που ασκούνται στο επιγονατιδομηριαίο μηχανισμό.
Όταν υποχωρήσει η φλεγμονή και το οίδημα το επόμενο βήμα είναι η ισχυροποίηση των μυών της περιοχής, ιδιαίτερα του τετρακέφαλου μυός, που έχει αποδειχθεί ότι παίζει σημαντικό ρόλο στην αποκατάσταση αυτού του προβλήματος. Χρήσιμη είναι η εκπαίδευση με Biofeedback. Το πρόγραμμα συνδυάζεται με ασκήσεις διατάσεων ώστε να βελτιωθεί η ελαστικότητα και η λειτουργικότητα των μαλακών μορίων της περιοχής. Τέλος το πρόγραμμα ολοκληρώνεται με ασκήσεις ιδιοδεκτικότητας.
Σημαντικό μέρος της θεραπείας είναι η ενημέρωση και η επανεκπαίδευση του ασθενή ώστε να προλαμβάνει τυχόν νέα υποτροπή του προβλήματος στο μέλλον. Περιλαμβάνει επανεκπαίδευση στην σωστή στάση, συχνά διαλείμματα κατά την διάρκεια δραστηριοτήτων που επιβαρύνουν τις αρθρώσεις των γονάτων, πρόγραμμα ασκήσεων, κολύμπι, ενώ καλό είναι να αποφεύγεται η άσκηση με ποδήλατο.
Παράλληλα με την ανάπαυση και τη φαρμακευτική αγωγή (αναλγητικά, αντιφλεγμονώδη) του ορθοπαιδικού, κρίνεται επιτακτική η ανάγκη για φυσικοθεραπευτική αντιμετώπιση που επικεντρώνεται στα παρακάτω:
• Φυσικά μέσα (tens,E.M.S., laser) για την ανακούφιση των συμπτωμάτων και τη μυϊκή ενδυνάμωση (έσω πλατύ).
• Κινητοποίηση επιγονατίδας (ολισθήσεις) και γόνατος στα όρια του πόνου.
• Μάλαξη γειτονικών μυϊκών ομάδων.
• Ενδυνάμωση τετρακεφάλου με έμφαση στον έσω πλατύ, για την ευθυγράμμιση της επιγονατίδας. Ισομετρικές και ισοτονικές ασκήσεις σε κλειστή-ανοιχτή αλυσίδα σε σετ των 10 επαναλήψεων.
• Ασκήσεις ιδιοδεκτικότητας γόνατος.
• Κρυοθεραπεία. Μπορούμε να κάνουμε παγομάλαξη ή να τοποθετούμε ψυχρά επιθέματα τυλιγμένα με πετσέτα για 10 λεπτά. Φροντίστε να επαναλαμβάνετε τη διαδικασία έως και 8 φορές μέσα στη μέρα.
• Τεχνικές περίδεσης της περιοχής με ελαστικό επίδεσμο ή άλλα είδη taping.
Η κολύμβηση είναι πολύ καλή αθλητική δραστηριότητα για άτομα με χονδροπάθεια επιγονατίδας, λόγω των μειωμένων φορτίσεων που δέχεται η άρθρωση του γόνατος. Αντιθέτως δραστηριότητες που προκαλούν πόνο όπως η άνοδος-κάθοδος σκάλας θα πρέπει να αποφεύγονται.
• Φυσικά μέσα (tens,E.M.S., laser) για την ανακούφιση των συμπτωμάτων και τη μυϊκή ενδυνάμωση (έσω πλατύ).
• Κινητοποίηση επιγονατίδας (ολισθήσεις) και γόνατος στα όρια του πόνου.
• Μάλαξη γειτονικών μυϊκών ομάδων.
• Ενδυνάμωση τετρακεφάλου με έμφαση στον έσω πλατύ, για την ευθυγράμμιση της επιγονατίδας. Ισομετρικές και ισοτονικές ασκήσεις σε κλειστή-ανοιχτή αλυσίδα σε σετ των 10 επαναλήψεων.
• Ασκήσεις ιδιοδεκτικότητας γόνατος.
• Κρυοθεραπεία. Μπορούμε να κάνουμε παγομάλαξη ή να τοποθετούμε ψυχρά επιθέματα τυλιγμένα με πετσέτα για 10 λεπτά. Φροντίστε να επαναλαμβάνετε τη διαδικασία έως και 8 φορές μέσα στη μέρα.
• Τεχνικές περίδεσης της περιοχής με ελαστικό επίδεσμο ή άλλα είδη taping.
Η κολύμβηση είναι πολύ καλή αθλητική δραστηριότητα για άτομα με χονδροπάθεια επιγονατίδας, λόγω των μειωμένων φορτίσεων που δέχεται η άρθρωση του γόνατος. Αντιθέτως δραστηριότητες που προκαλούν πόνο όπως η άνοδος-κάθοδος σκάλας θα πρέπει να αποφεύγονται.



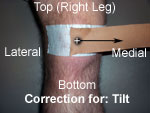 Lateral tilt component is corrected by pulling the tape from the midline of the patella medially.
Lateral tilt component is corrected by pulling the tape from the midline of the patella medially.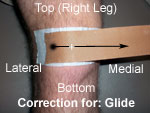 Excessive lateral tracking is corrected by pulling the patella medially.
Excessive lateral tracking is corrected by pulling the patella medially. Excessive external rotation of the patella is corrected by taping from the middle inferior patellar pole upward and medially.
Excessive external rotation of the patella is corrected by taping from the middle inferior patellar pole upward and medially.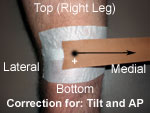 An anteriorposterior tilt of the patella is corrected by attempting to tilt the inferior pole of the patella anteriorly by placing a strip of tape at the superior pole of the patella and pulling the tape medially.
An anteriorposterior tilt of the patella is corrected by attempting to tilt the inferior pole of the patella anteriorly by placing a strip of tape at the superior pole of the patella and pulling the tape medially.